
[B]URLINGTON — Officials from the University of Vermont Health Network are asking state regulators to increase the budget for two of its largest hospitals by 3.5 percent for next year.
Under the proposed budget, the UVM Medical Center in Burlington and Central Vermont Medical Center in Berlin would collect combined patient care revenue of $1.4 billion in 2018, an increase of around $47.5 million over last year.
The Green Mountain Care Board primarily regulates how much patient care revenue hospitals can earn, before expenses. The board also regulates the prices that hospitals are allowed to charge commercial insurance companies for services.
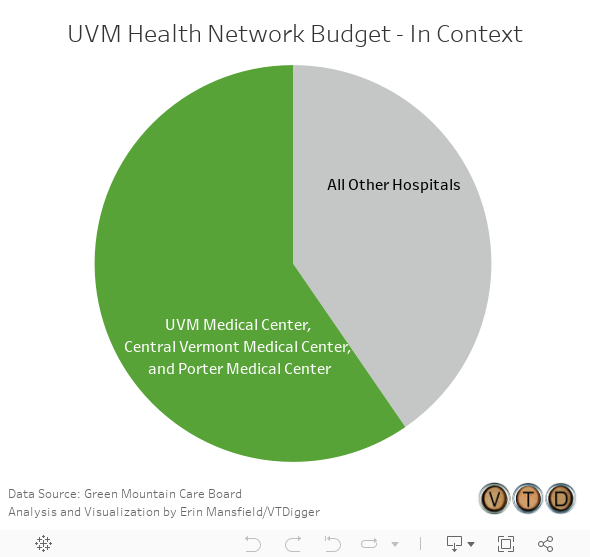
The UVM Medical Center’s proposed budget accounts for $1.2 billion of the $2.5 billion in patient care revenue that regulated hospitals are asking to receive. Central Vermont Medical Center’s budget is another $198.7 million, and Porter Medical Center’s budget is $78.7 million.
Additionally, UVM Medical Center and Central Vermont Medical Center are proposing to increase prices for insurance companies by just .72 percent because the hospitals went over budget in fiscal year 2016. Porter Medical Center is proposing to keep prices flat.
However, Porter Medical Center, which joined the UVM Health Network in the spring, is not part the larger network’s budget proposal this year. Additionally, the network’s three hospitals in New York are not included in the budget, according to Michael Carrese, the spokesperson for UVM Medical Center.
UVM Health Network officials said the most important part of the budget proposal is that it shifts focus from providing “sick care” — that is, on procedures, pharmaceutical drugs, and other services people need when they’re already sick — to keeping people healthy and out of hospitals by emphasizing primary care and community health initiatives.
The budget proposal lists a variety of approaches to improving population health, such as investing in affordable housing, educating people about nutrition, helping them get healthy foods, and increasing access to mental health and substance abuse services.
The budget also proposes to spend $196.2 million on capital investments in fiscal year 2018, including $45.5 million on its new inpatient building, which will offer patients private rooms instead of shared rooms starting in 2019; and $44.6 million on a proposed network-wide electronic medical record system, which has not yet received regulatory approval.
The network plans to spend an additional $25 million to acquire property in South Burlington, a project that will require regulatory approval; $7.7 million to replace the Essex Adult Primary Care building in Essex Junction; and $2.5 million to update and expand the Vermont Cancer Center, “to accommodate patient needs.”
The network plans to spend $2.9 million on new radiology equipment. The network is also “ in the early planning stages” of spending $1.5 million in fiscal year 2018 on new equipment for storing medical images.
Carrese said that this is the first year the network’s hospitals have submitted a joint budget proposal. Compared to the two hospitals’ recent separate budget increases, this year’s increase represents somewhat slower growth, he said.
In 2016, UVMMC requested a 3.6 percent budget increase and Central Vermont Medical Center requested a 4.7 percent increase, Carrese said. In 2017, UVMMC requested a 4.1 percent increase and CVMC requested a 10.3 percent increase, he said.
Carrese said 40 percent of the 2018 revenues are set to come from lump-sum payments, or an arrangement where health care providers receive a monthly payments to treat a certain number of patients. The idea is to change the incentives for health care providers so that they will emphasize preventive care instead of “sick care.”

Todd Keating, the network’s chief financial officer, told the board he was excited to work under this new system. He said the change in paradigm should remove the perverse financial benefit of many people getting sick.
Robin Lunge, another board member, said she was concerned that “changing the financial incentive is necessary, but it’s not sufficient for success.”
Lunge said she was concerned that changing operational habits away from a quota mentality would be “a really big shift” for hospital administrators, especially chief financial officers.
Keating said he didn’t think that would be much of a problem.
“For my entire career, presenting to finance committees and boards and everything, I’m sitting there saying ‘We had a great month because we had a flu outbreak,’” Keating said.
“I would love to be able to go to my finance committee and board and say ‘We had a great month because we had an outbreak of health,’” he added.
“Changing to population health management changes that parameter totally” so that “keeping people healthy makes your bottom line stronger — which is the way it should be,” Keating said.