Editor’s note: This commentary is by Robert Holland, MD, MS, who is a physician and policy analyst who lives in Irasburg. He is employed by North Country Hospital as an emergency department physician.
Beginning Aug. 20 in public hearings the Green Mountain Care Board will review the budgets of Vermont’s 14 hospitals. Though there is no screenwriter for this annual ritual, the actors are well known and their scripts are predictable. As the proposed budgets overall are not far from the requests of the GMCB any differences between requested and approved will be in the domain of tenths of a percentage point. The overall context of these discussions, namely Vermonters’ hospital costs versus hospital costs in other states and around the world, will not be mentioned.
An important factor influencing hospital costs is the wealth of the community it serves. The figure below displays the per capita annual hospital costs compared to the per capita income for all 50 U.S. states and the District of Columbia for the year 2014. Though the data is four years old there has been no dramatic changes that would call for significant changes in the pattern displayed.
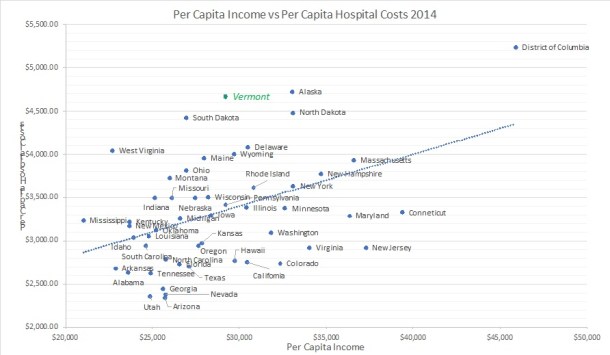
In 2014, only Alaska and the District of Columbia had higher per capita hospital costs than Vermont. The dotted line represents the predicted hospital costs based upon the known per capita income using standard statistical techniques. Vermont has the highest vertical distance above the dotted line. States above the line have factors increasing hospital costs other than per capita income. Though Alaska and the District of Columbia have higher per capita hospital costs, those costs are a smaller proportion of per capita income. Vermonters pay 16 percent of their per capita income on hospital costs while Alaska and D.C. citizens spend 14 percent and 11 percent respectively. Vermonters have a very high burden of hospital costs; only two other states have a higher burden of hospital costs, South Dakota (16.4 percent) and West Virginia (17.7 percent). Over the interval of 1991 through 2014 Vermont had an average annual hospital growth rate of 7.7 percent — the highest in the United States – and most likely the highest on the globe.
This legacy of the highest hospital cost growth rates in the United State for 23 years has adverse effects on the Vermont economy. In 2014 the U.S. health sector consumed 15 percent of the gross domestic product; in Vermont, it consumed 20 percent of the gross state product. If Vermont’s hospital costs had grown at the national rate of 5.7 percent rather than 7.7 percent annually over the 1991-2014 interval, in 2014 Vermont citizens would have been spending $1.886 billion on hospital care rather than $2.926 billion, saving $1.016 billion – 3.7 percent of the Vermont gross domestic product of $26.99 billion.
The goal of bending Vermont’s cost curve down as expressed by the chair of the GMCB and explicitly embedded in the all-payer agreement with the federal government and the goals of OneCare Vermont – namely, limiting growth rate to 3.5 percent annually protects health care’s large bite out of the Vermont economy. Is there an alternative?
According to Donald Berwick, MD, previous administrator of the Center for Medicare Services, waste in health care spending is estimated to range from a low of 21 percent of all health care spending to a high of 47 percent with a midpoint of 34 percent (JAMA 2012;307(14):1513-1516). Is there evidence of waste in Vermont hospital care?
I studied 2016 Vermont data sets of emergency department visits and outpatient visits for the primary diagnoses associated with sore throats. When these diagnoses are the only diagnosis submitted for billing, people present to a health care facility and undergo a brief history and physical examination and a rapid test for streptococcal infection. If they prove to have a streptococcal infection they are given a prescription for an antibiotic and instructions on how to treat the associated symptoms. If the strep test is negative they are given the instructions only. The fundamental idea underlying this analysis is that people with a common sore throat do not need the expensive services of a hospital emergency department; they need timely and cost-appropriate-to-value access to primary health care. The data sets record relevant parameters for 269,862 emergency department visits and 1,558,082 outpatient visits in 2016. There were 3,914 emergency department visits for simple sore throat with average charges of $835, total charges $3,266,984. There were 16,711 outpatient visits for simple sore throat with average charges of $108, total charges $1,812,014. Eighty-seven percent ($2,834,038) of total hospital emergency department charges for pharyngitis ($3,266,984) are waste; 56 percent of health system charges for these diagnoses are waste.
The principle is clear — reimbursement should reflect the value of the service provided and not the charges of the hospital. No leaders are calling for major changes from the status quo of moderating health care cost increases. No extant political force is strong enough to oppose the status quo. Any leader who wants to effectively address affordability for Vermonters must address waste in health care. More than 20 countries have higher population health than Vermont while spending only 10 percent of their gross domestic product on health care. Given the quality of community in Vermont we should be able to provide high quality population health for 15 percent of gross state product freeing up about $1.35 billion annually in 2014 dollars for productive use. The missing ingredient is leadership.

