
[F]or Gov. Peter Shumlin’s payroll tax proposal to succeed it will need the approval of the House Ways and Means Committee, where support appears tepid.
Shumlin wants to levy a 0.7 percent payroll tax on all businesses in the state to increase the amount Medicaid pays doctors and hospitals and to make other investments in Vermont’s health care system. The governor has said the proposal will reduce the growth in private health insurance premiums by 5 percent. That’s because Medicaid currently pays roughly 60 percent of what medical care costs, and providers make up the difference by negotiating higher payments from private insurance, a cycle known as the Medicaid cost shift.
Vermont’s regulated health care industry and buy-in from stakeholders will help ensure that shoring up Medicaid reimbursements will lower premiums, according to administration officials. So will targeting Medicaid rate increases for specific services designed to “maximize” the amount of money regulators can help insurers recover from providers and pass on as savings to their customers, said Michael Costa, deputy commissioner of Health Care Reform.
The question is whether the premium savings to businesses will offset what they pay through the payroll tax. That depends greatly on whether a business offers health insurance in the first place, and what percentage of their payroll goes toward offering that benefit.
“As you know, there are winners and losers in any tax policy,” Costa told members of the Ways and Means Committee on Wednesday.
“Yes, but we want more winners than losers,” responded Rep. Janet Ancel, D-Calais. For her committee to support the payroll tax, it would need to be confident that would be the outcome, Ancel said.
In an interview on Monday, House Speaker Shap Smith said before the House can “even think about” supporting the payroll tax, lawmakers would need to have a much better understanding of how any money raised would be returned to premiums. “I don’t think we have an answer to that yet,” Smith said.
Figures from the legislative Joint Fiscal Office show that, assuming health care spending grows 6.1 percent (a consensus figure for next year with the administration), the “break-even point” for businesses would be 14.5 percent of payroll spent on employee health care, if the governor is able to deliver the 5 percent savings. The break-even point rises to 17 percent of payroll at 4 percent savings and 23 percent of payroll at 3 percent savings. The average business in the state pays 11.45 percent of payroll toward health care, according to figures from the Green Mountain Care Board. But both legislative and administration officials said the average is a crude instrument, because there is wide variance in what businesses pay, and many don’t offer coverage at all.
If the growth in health care spending exceeds estimates, the savings would be squeezed.
Rep. Adam Greshin, I-Warren, said, “It just shocks me how razor thin the margin for error is on this.”
Rep. Jim Masland, D-Thetford Center, agreed, repeating Greshin’s “razor thin” remark.
Shumlin’s payroll proposal generates $41.4 million in FY 2016, and close to $90 million going forward on an annualized basis. That money leverages a federal match of $86.1 million in FY 2016, and $190 million on an annualized basis going forward.
The proposal includes $15.9 million in nondiscretionary spending to cover the state’s expansion of Medicaid through the Affordable Care Act, as well as a statutory increase in payments to nursing homes. There are 58,000 Vermonters new to Medicaid, according to state figures, which includes close to 37,000 who were previously covered by the Vermont Health Access Plan, a state health coverage program similar to Medicaid, leading Shumlin administration officials to peg the number of new Medicaid beneficiaries at closer to 21,000.
If Ways and Means rejects the payroll tax, that money would need to come from another source, or lawmakers would need to reduce Medicaid rates to cover the newcomers.
House Speaker Smith says he believes reducing the impact of the Medicaid cost shift on insurance premiums is the right thing to do, and there may be other ways to raise the money.
“The reality is the cost shift is a tax right now,” Smith said. “It is a tax to all businesses that provide health care coverage, it’s just hidden, and if people feel they’d rather have a hidden tax than one they can see we’ll continue to do that.”
Smith suggested that the money could be raised through yet-to-be determined sources, such as increasing the claims assessment (a tax on health care claims) and the employer assessment (a flat fee for each worker companies do not provide insurance for).
The rest of the money in the governor’s proposal would pay for the targeted increases in Medicaid rates, increased payments to providers that participate in the Blueprint for Health managed care program, increased payments for home health services, reduced out-of-pocket costs on the exchange and helping Vermont apply for a federal waiver to set Medicare payments.
Lawmakers on the House Health Care Committee must choose which of those initiatives, or others put forward by the committee, they believe are worthwhile to pay for, with whatever amount the money committees (Appropriations and Ways and Means) make available.
Rep. Kiah Morris, D-Bennington, said a variety of the governor’s proposals have resonated with her and other members of the committee, including addressing the cost shift, increasing Blueprint payments and supporting home health services. But “no one bill is likely to make it out intact” from the committee, which she believes will settle on a combination of the governor’s proposals and proposals from committee members.
Morris said she worries that people are too focused on whether the governor can deliver savings to businesses and premium payers in the near-term, and not whether addressing the cost shift by increasing Medicaid rates is the right long-term policy choice.
Even if the governor’s proposal makes it intact through the House, there are a litany of timing issues — not to mention winning Senate approval — that complicate its execution.
Al Gobeille, chairman of the Green Mountain Care Board — Vermont’s health care regulatory body — said Shumlin’s payroll proposal can only succeed in reducing the growth in private premiums next year if the administration can say by April what Medicaid rates will be for specific services.
“There are requirements we will place on DVHA that if they can’t meet, we can’t do this,” he said, referring to the Department of Vermont Health Access, which runs Vermont’s Medicaid program.
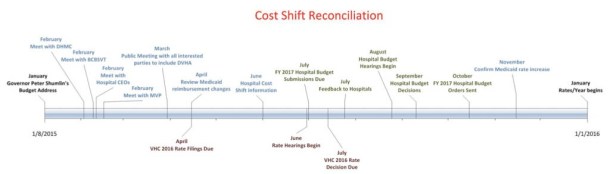
April 15 is a crucial date, because that’s when Blue Cross Blue Shield of Vermont and MVP Health Care will submit rate requests for insurance plans offered through the Vermont Health Connect exchange. The board needs to know by then how DVHA plans to apportion the rate increase across Medicaid services, Gobeille said, so that it can adjust and approve insurers rates in July.
Vermont’s hospitals have agreed to submit their budgets a month early in June, so they can be adjusted to reflect the increased Medicaid rates as well.
Robin Lunge, director of Health Care Reform, said DVHA will be able to deliver, but will likely provide the board with a range of possibilities based on what’s in play at the Statehouse. By April, legislation will likely have passed the House, and the administration would have a sense of where things are going in the Senate. That will allow them to present the board with a number of likely scenarios for how the Medicaid rate increases will be apportioned.
Provided all those dominos fall into place, Gobeille said the premium reduction Shumlin is promising businesses for going along with the payroll tax could all be scuttled by utilization.
If people use more medical services than anticipated savings could materialize, but would be subsumed by higher spending. Utilization of health care services is beyond the direct control of regulators, health care providers and the administration, though many of Vermont’s ongoing health reform initiatives — and many of the ones in the governor’s payroll proposal — seek to reduce the volume of services by improving patient health and changing financial incentives in medicine.
Gobeille has told lawmakers he’s not willing to guarantee success, but he has said he believes it’s possible.
“Right now, we have a lot of people willing to put their shoulder to this,” he said.
Editor’s note: Anne Galloway contributed to this report.