
The Deeper Dig is a weekly podcast from the VTDigger newsroom. Listen below, and subscribe on Apple Podcasts, Google Play, Spotify or anywhere you listen to podcasts.
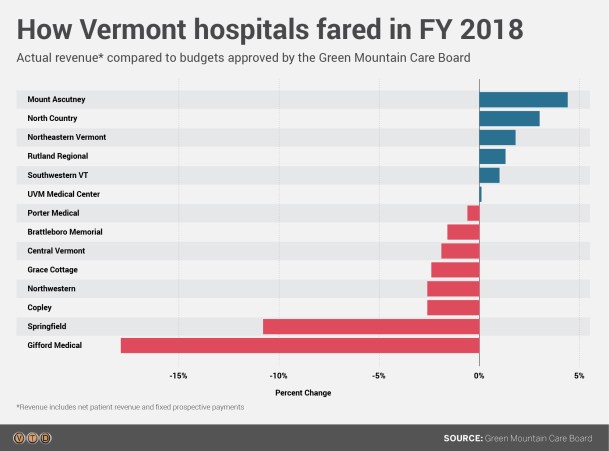
[S]pringfield Hospital’s financial woes late last year led to the ouster of their management team and a bailout by the state. But new data released by the Green Mountain Care Board last week shows that Springfield is hardly alone: A majority of hospitals in the state operated at a loss in the last fiscal year.
The care board’s leader Kevin Mullin said the trends are a “huge concern.” Expenses are growing faster than revenues across the system.
“If you don’t have a margin, you don’t have a mission,” Mullin said this week.
Mullin and other officials peg the disparity to broader trends that can’t easily be solved through regulation. Vermont’s demographic decline is starving hospitals of qualified staffers, causing them to reduce patient loads and hire expensive temporary workers. And as local economies decline, hospitals see more patients who use Medicare and Medicaid insurance, which means they receive less revenue. Medicaid reimburses at roughly 60 percent of providers’ costs; Medicare rates are at about 80 percent of cost.
Demographic shifts are hitting rural areas across the country. “It’s a mega trend, not just a Vermont thing,” said Al Gobeille, the secretary of the Agency of Human Services and the former chair of the care board.
“Some of our communities are shrinking, and are projected to shrink by large numbers over time,” Gobeille said. “What does that mean to the institutions in those areas?”
Gobeille and Mullin both see potential in rural hospitals coordinating specialists across locations, or affiliating with larger, more stable hospital systems. Mullin sees the state’s all-payer reform project, which rewards hospitals based on health outcomes, as a more sustainable than a fee-for-service system. But in the short term, hospitals operating in the red will likely need to make cuts to balance their budget woes.
On this week’s podcast, Gobeille and Mullin describe the pressures facing Vermont hospitals. VTDigger’s health care reporter Mike Faher discusses the data on hospital finances. And Katy Savage describes the situation at Springfield.
[showhide type=”pressrelease” more_text=”Read full transcript” less_text=”Hide full transcript” hidden=”yes”]
Katy Savage: Hello?
Hey, Katy, it’s Mike from Digger. How’s it going?
Savage: Hi, Mike. Good, how are you?
I’m good.
Katy Savage lives in Chester. Since last fall, she’s been reporting for VTDigger on the financial collapse at Springfield Hospital.
Savage: Back in, I guess December it was, a doctor walked into his office one morning and found that there was no heat in the building. They called the heating company to come and fill the oil. They told him they weren’t going to fill it because Springfield Hospital hadn’t been paying them. Then I found out that there were some employees who weren’t getting their health insurance paid by Springfield Hospital. And there were some other vendors that weren’t being paid. That’s how it started.
Had there been any other indications that the hospital was having financial issues?
Savage: Not that I was aware of. I knew that they were looking at changing the contracts for the emergency room. And that had made a lot of people in the community really upset because the emergency room had been there for 40 years. The hospital basically said that they were looking at all of their contracts and trying to save money, as much money as they could. They are even looking at like copier contracts and like, light, you know, heat and electricity. Wherever they could find savings. And it just sort of unraveled this whole thing as to, there was a much bigger issue going on there.
The CEO and CFO abruptly left the hospital within like a month of each other. I later learned that this CFO had been fired, and it’s still unclear why the CEO left. So they were looking at rearranging the whole upper management, and they were looking at basically every single service line to find ways to save money.
When did you start to get a sense of the scope of that issue?
Savage: You know, when the audit report came out, this was sort of recently, it showed that they lost $14 million in two years. I think that that was sort of a shock to a lot of people. I don’t think that anybody really realized how bad it was.
In January, the state loaned Springfield Hospital $800,000 to make sure it wouldn’t close. State officials say Springfield Hospital had management issues that made their financial problems worse. But the root causes were trends that go way beyond that one location.
Mike Faher: I think it’s an extreme example, but it’s also not uncommon based on what we’re seeing elsewhere.
Mike Faher is VTDigger’s healthcare reporter. Last week, he reported on new data from the state’s healthcare regulators, the Green Mountain Care Board, that showed that a majority of hospitals within the state are operating at a loss.
Faher: Statewide expenses year to year are growing at a faster rate than the revenues, and at the same time, their operating margins are decreasing pretty much year after year. That’s not sustainable.
Most of these hospitals that did lose money ended up still in the black because they have investment income, non-operating income it’s called, that they can use to get back out of the red. But that also can’t go on forever, reserve spending can’t go on forever. So the really troubling trends that a lot of people are seeing here is that this kind of spending and revenue, it just can’t continue.
So you’ve been talking to members of the Care Board, to other officials, about these trends. What are they telling you?
Faher: I think that certainly the chairman of the Care Board sees it as a workforce issue. I see that myself in reading hospital budget reports. Workforce hits hospitals in several ways, you know on one hand they have to pay exorbitant, really, amounts for traveling nurses and temporary doctors just to fill their staffs, and on the other hand, you don’t have the staff, especially in terms of doctors or surgeons, to handle the traditional patient volumes you would have, and so you lose money, you lose revenue. You’re spending more and you’re losing revenue. And so workforce, it just seems like such a big deal because it really takes a huge toll, especially on small hospitals, which we have quite a few of in Vermont.
Kevin Mullin: There’s the expense pressures, and there’s the revenue pressures. If you don’t have a margin, you don’t have a mission.
This is Kevin Mullin, the chair of the Green Mountain Care Board.
Mullin: What we’re seeing from hospitals as they come into their budgets, they’re paying twice as much for a traveler or locum as they would if they had an actual nurse employed there or an actual tech employed there an actual doctor employed there. And so, to think that we’re not incurring costs from our failure to address our workforce shortage, we are paying that cost, and everybody’s paying it in the form of the cost that they’re paying for their insurance, or the cost of their procedures that they have. So you know, it’s a hard place that we’re in right now. And if we don’t address the workforce issue, I think there are going to be more stories like Springfield rather than less. And that scares the heck out of me.
There are other factors affecting Vermont hospitals’ bottom lines: an increase in mental health patients, capital costs, like upgrading old buildings and equipment. But it’s also just getting more expensive to operate hospitals in rural parts of the country.
Mullin: If you’re in an area that doesn’t have a strong local economy, you’re not going to have much for commercial payers. And that is very problematic. If you’re getting most of your revenue from government payers, which most Vermont hospitals are now, is problematic. Because now Medicare is below the actual cost and Medicaid is below that.
Gotcha. So when it all adds up, in a community where more people are on Medicare and Medicaid, that’s hitting the hospital a lot harder on their bottom line?
Mullin: A lot, lot harder.
Al Gobeille: I think that when you look nationally, you’ll see that small hospitals are struggling. And we’re not immune to that here in Vermont.
This is Al Gobeille, the head of the Vermont Agency of Human Services, and the former chair of the Care Board.
Gobeille: Each critical access hospital is going to have to assess where it’s at, what it’s delivering to the community and how it’s integrating with other providers. And, you know, that is happening in New Hampshire, that’s happening in New York, and that’s happening all across the country. It’s a mega trend, not just a Vermont thing.
Al said there are broader demographic trends putting pressure on Vermont hospitals.
Gobeille: You know, we’re getting older, grayer, and some of our communities are shrinking, and are projected to shrink by large numbers over time. And so when you see colleges closing, when you see Act 46 and school mergers and all the tension with that, that’s the same — that’s going to affect all of our institutions, that’s going to affect our hospitals, our schools, colleges. That’s why that is such an awesomely powerful both conversation and problem that we have to face as a state.
And it’s interesting, especially with this issue, because I know one thing the Care Board has isolated as this broader pressure is workforce, and having people to staff these hospitals, and it seems like those two kind of aspects of it are almost exacerbating each other.
Gobeille: Yeah. So, you know, if if I told you 25 years ago we were going to have a two and a half percent unemployment rate, you would have said, wow, that’s going to be a great thing for the state. But, you know, it’s really one of those things where, wait a minute, there’s a whole story here with the two and a half percent. Every meeting I go into with my team, corrections, Department of Mental Health, nursing homes, you know, whatever. Everyone says, we have a workforce problem. And the truth of the matter is, it’s this larger Vermont problem, this larger demographic problem of Vermont has a workforce problem. And so it’s absolutely impacting hospitals and every other business in the state. No one is immune to it.
Kevin told me that one of the state’s challenges now is trying to keep hospitals stable using a limited set of regulations.
Mullin: What we have to keep pointing out is that we as a board don’t have the tools to go in and manage a hospital. People say well why didn’t you go in and and make changes at Springfield? All we can really do is make suggestions and hospitals are run by their local boards, they’re all not for profit hospitals, we don’t have a for-profit hospital. It’s interesting at times to listen to some of the comments when we have public comment periods, because so many people talk about the great profits that hospitals are making, and it’s just not the case.
You say that you don’t have the tools to actually stop this from happening. Do you think the system would work better if you did? Do you think that’s power the Care Board should have?
Mullin: No. I think that would be an overstep by government. I think that what we want to make sure in government is that people have access to quality medical care at a price that they can afford. But I don’t think that we should be running our hospitals or doctors offices. I think that would be a huge overstep, and it might end up in worse results than what we see now.
Do you think there are changes that should be made to how the regulatory process works that would prevent a situation like a Springfield happening again?
Mullin: Well, I absolutely do think, and we’ve already, you know, been tweaking our process. You know, one of the things that we had always relied on is openness and transparency, and the truthfulness of data that is submitted to us and now we’ve made changes so for example, if they’re having an inability to pay bills, they have to notify us, if they have a change in staff at the executive level, they have to notify us. We’re continuing to try to fine tune the process to try to find that sweet spot where we’re doing the right amount of regulation but not creating additional costs and burdens on our community hospitals because of what we’re doing. Hopefully we’ll find that right spot, who knows.
Faher: The Green Mountain Care Board regulates insurance rates, they regulate hospital budgets. It’s an annual thing where the hospitals come before the Care Board and say, for the next fiscal year, we want to earn X amount of money. And we want to charge insurers an average of X amount. And those are the two sort of leavers that the Care Board has. And generally, from what I’ve seen in my short time on the health care beat, the Care Board will grant hospitals an increase in the revenue they can earn the next year and they will grant hospitals an increase in the rate that they can charge insurers, but they will cut both of those requests and a lot of cases from what the hospital wanted.
So it’s kind of a negotiating process almost.
Faher: It is. It is in the sense that, you know, the there’s a request and then there’s there’s debate, but at the end of the day, the Care Board’s order is what it is.
What happens if these declines keep happening and more hospitals get into the situation that Springfield was in? Where they’re really on the brink of closure?
Faher: You know, the state can’t afford to bail them all out like they did with Springfield, at least I don’t think they can. I’m not sure they would want to, you know, last year when I interviewed the chairman of the Care Board, he made sort of a radical suggestion, which was, in the long term, maybe not every hospital can provide every service. It may not be possible.
Mullin: Not every hospital can do a heart operation. So they have to make those type of decisions. With that being said, if they’re not going to provide certain functions at their local hospital, the residents of that area have to know that they’re going to get those functions provided. So if you need heart surgery, you need to know that you’re going to get into either a UVM, or a Dartmouth or an Albany to make sure that you get what you need.
Faher: We might have to think about what services really make the most sense in which areas, but that’s really hard for a community. If you’re a resident in a rural community, you don’t want to think about having to drive, I don’t know, 50 miles or more for a major or even a minor treatment that suddenly is no longer available at your hospital. But we’re seeing that, you know, Springfield just decided to close their birthing center. And that’s another thing that we might see happen. Hospitals might be forced to start picking and choosing, what can we do and what can’t we do in order to keep our doors open. I don’t mean to sound so dire, but the cost pressures are so real that I’m not sure that I see any way, any other way out of it.
Mullin: Springfield recently made the decision to close their birthing center. Birthing centers are not a moneymaker. But no community ever wants to give up that. It’s usually a very, very painful decision, as it was in Springfield, a very painful decision. On the same token, if you were trying to find any upside out of that, it could actually help Brattleboro, who still does birthing. Because they’re not making money, but now they might lose less if they have a few extra births that are occurring there each month. So collaboration is key.
Faher: One other thing I haven’t mentioned is that hospitals can, they can merge, they can get taken over. Mount Ascutney Medical Center in, I want to say, Windsor, they’re an affiliate of Dartmouth Hospital. We’ve seen Dartmouth and UVM Health Network affiliate some hospitals in recent years, that’s another way that a small independent hospital can try to dig their way out.
Gobeille: You know, it’s almost like you can’t go it alone anymore. You know, it’s really hard to go it alone. And so, you know, Porter made a decision to affiliate. And, you know, now, Porter’s flourishing. And so I think the real lessons to learn are maybe from a Porter, not from a Springfield.
Do you think we’re going to see more of that? Those types of mergers and affiliations?
Gobeille: We’re seeing we’re seeing it all over the United States. I mean, just in New Hampshire, we just saw Dartmouth, you know, merging with another health system and, you know, other critical access hospitals wanting to and here’s the key point here is the critical access hospitals, the smaller hospitals, approach the bigger hospitals, the bigger hospitals aren’t. We met with Dartmouth, they’re not out, you know, because often it’s a financial drain on the big hospital. Sure. It’s not what most people think. But, you know, they’ve got to subsidize the smaller hospital to try to keep care in the community. And it’s these nonprofit hospitals’ mission to do that. But it can be, financially a challenge.
But that seems like a trend that that could be coming here more?
Gobeille: I think that’s a trend. Yeah. If you think out five years, you know, and you say, if Rutland was to actually see a 10 percent, or 12 percent reduction in population, or Bennington 5, 6, 7 percent in the next 5, 10 years, what does that mean to the institutions in those areas? Hospitals are just one of the institutions. And so you know, you’ve got to start thinking about all sorts of shared services, all sorts of integrations that you’d have to do to make it work. It’s a lot easier to grow as a town, city or state, than it is to shrink. Shrinking’s hard. And we are going to face some real difficult challenges over the next five to 10 years if that’s what really happens. And that’s sort of that’s what’s forecast to happen. And so what I see happening over the next five years is a lot of working together to make sure that people have the services they need in their community.
Faher: I think in the short term, the only, I hate to say it’s a solution, but the thing that hospitals have to do, it seems, is cut their costs. And we’re seeing that with Gifford. In addition to asking for more revenue from the Care Board, they they’ve cut something like a million plus out of their budget over the past year. And I think we’re going to see other hospitals doing the same thing. Because the solutions that could bring more revenue, they’re not quick.
The last thing I would mention is that there is this massive health care payment reform effort, the all payer model. It’s really complicated, and it’s just so, it’s hard to say whether it’s going to really change things. But it’s got a sort of dual pressure on hospitals right now. On one hand, they’re investing in it. They’re paying money to support it. On the other hand, the idea is that long term, we don’t pay so much for every test and every procedure, and we start paying to keep people well, we start paying for health outcomes. And if that works, if that can somehow happen in a really meaningful way, that could have a huge impact on hospitals, because they could, they could really start to do some pretty innovative things with their rural populations to try to keep them healthy. And maybe they don’t have to offer every intensive service under the sun.
Mullin: In the past, doctors and hospitals measured success on the revenues that were coming in the door, so it was more volume, more volume, more volume, you know, more tests, more procedures. And we know from studies from Dartmouth, from people like Elliot Fisher and Jack Wennberg over there, that more care doesn’t necessarily equate into better outcomes. So you need the right amount of care and you need to make sure that there’s access to the right care. This new experiment that Vermont is undergoing, the all-payer model, is a move to try to incent providers to try to keep people healthier.
The all-payer model brings up this kind of, it seems to me like sort of a paradox where that seems like it could result in great outcomes for the patient. But for a hospital that’s struggling to bring in revenue, you know, if there are fewer procedures being given, fewer patients in their care, that that would be quite a challenge for them.
Mullin: And that’s why the fixed perspective payments are a help. Because if they’re really good at managing that care and bringing down the expenses of the population that they’re serving, then they could benefit in that revenue. So there’s a risk corridor, and they could benefit to a small degree if they’re doing really good work. But of course, it is a fear, because the last thing that we want is for a hospital to come into a budget approval hearing and say ‘we had a really good year last year because we had more people in the hospital with flu or, or what have you.’ And so, to me, that’s not a really good year, it might be a good year revenue-wise, but it’s not a good year for really what we’re focused on, which is the health outcomes of Vermonters.
But again, you know, if their revenue picture gets so bad that they risk closing, then that has really adverse effects, right?
Mullin: Especially in a fee for service world, because that that is the world that they would not be able to have any benefit. But if they’re able to share in some of the savings that could occur, then it may not necessarily have that same effect. But this is a slow evolution and you know, we’re very early on in our brave experiment to try to change the way people are cared for.
Faher: It’s this entire philosophical shift, theoretically, that really does reward, in a financial way, a hospital for keeping its patients healthy. And it works for primary care practices too, and it works for independent doctors, supposedly. But I think people are putting so much of their hope on that because the current system is clearly so messed up. And the current financial situation for hospitals is clearly so bad that it’s hard to see — it’s hard to see a way out of it. If you can imagine this massive paradigm shift in how hospitals are paid, that might be a way out of it. It’s just, we just don’t know whether it’ll work.
Thanks Mike.
Faher: Thanks.
Subscribe to The Deeper Dig on Apple Podcasts, Google Play, Spotify or anywhere you listen to podcasts. Music by Blue Dot Sessions.
[/showhide]