
An analysis by VTDigger shows that, although individual hospitals vary, Vermont’s 14 hospitals have, on average, improved their financial footing since the Green Mountain Care Board started regulating hospital budgets in fiscal year 2013.
Four hospitals — the University of Vermont Medical Center, Northwestern Medical Center, Mount Ascutney Hospital and Health Center, and Gifford Medical Center — have seen assets grow from fiscal year 2001 to 2016.
The six hospitals had enough cash on hand in fiscal year 2015 to cover costs for at least a six month period: Northwestern Medical Center (378 days), UVM Medical Center (201 days), North Country Hospital (199 days), Brattleboro Memorial Hospital (196 days), and Gifford Medical Center (188 days).
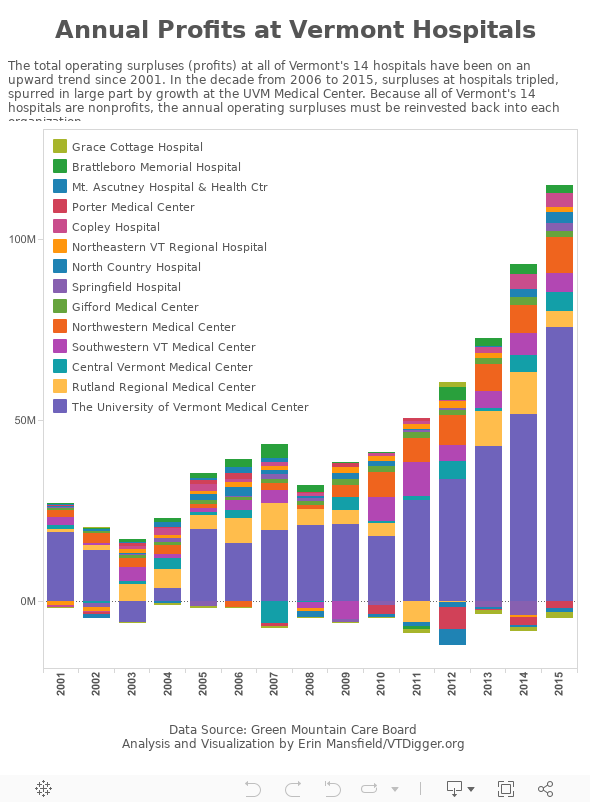
The total operating surpluses — also known as profits — tripled from $37.3 million in fiscal year 2006 to $110.4 million in fiscal year 2015. The average operating surplus over that time period went from $2.7 million to $7.9 million, driven largely by increased profits at the UVM Medical Center.
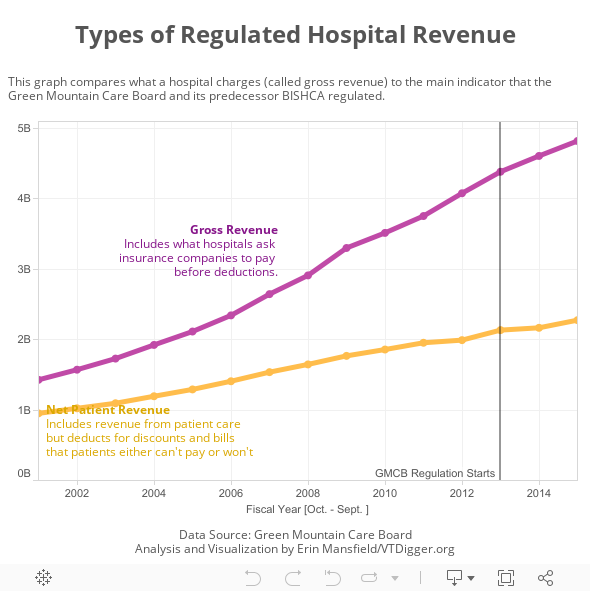
And while net revenue from patient care is down to about $2.3 billion annually, the amount that hospitals charge insurance companies for services has been approaching $5 billion.
“My concern is that nonprofits are behaving like corporations,” said Peter Galbraith, a former state senator from Windham County who is running for governor. “That’s not what a nonprofit is or is supposed to be.”
“What’s happening is that instead of keeping costs down—using the extra revenue, lowering prices, so that its focus is entirely on the service—the extra money is going into empire building and these outsized salaries,” Galbraith said.
The average hospital administrative salary in 2013 was $500,000.
Ken Libertoff, a mental health advocate, said Vermont hospitals “show an amazing degree of profit vigor,” despite being exempt from taxes, and said they “have clearly used resources to heavily compensate administrators at a level that greatly exceeds other Vermont industries.”
Libertoff said: “The cumulative impact of the reported operating surplus levels, current hospital assets and hospital cash reserves makes one wonder whether Vermont hospitals are becoming too big to fail, or to regulate.”
Mike Del Trecco, the vice president of finance for the Vermont Association of Hospitals and Health Systems, said hospitals have faced “downward pressure” on their patient care revenue, and it’s easy for the general public to misinterpret the budget numbers.
Del Trecco emphasized that hospitals, because they’re nonprofits, must reinvest profits back into their organizations. He said that most of that money goes back into paying for technology at hospitals, to the benefit of patients. He pointed to a recent experience with his own mother.
“When you’re there and you’re sitting there with your mom or your loved ones, you sort of take for granted all of the technology that can help with the diagnosis,” Del Trecco said. “At that point in time, I don’t care. It’s whatever it is to fix the problem.”
Surpluses/Profits
The role of hospital regulators
Hospital budgets have been regulated for more than two decades. In 1992, the Legislature passed a law giving regulatory power to a now-defunct agency called the Hospital Data Council.
Later, those duties moved over to a new agency, the Banking, Insurance, Securities, and Health Care Administration, and BISHCA spent the 2000s regulating the amount of revenue that hospitals receive from patient care — after making deductions for bills that patients either can’t pay or won’t pay.
Under BISHCA’s regulation, if the hospitals went over their revenue caps, BISHCA would tell them to lower their prices the following year, in essence paying back ratepayers for the excess revenue they took in the previous year.
By April 2012, when Vermont was moving full speed toward a single-payer health care model under Act 48, the Legislature split BISHCA into two entities—the Department of Financial Regulation and the Green Mountain Care Board.
Act 48 instructed the board to regulate hospital budgets such that they “promote efficient and economic operation of the hospital,” and “reflect budget performances for prior years,” among other things. The law also directed the board to collect information on hospitals’ administrative costs, and gave the board broad authority to define administration.
The board has since focused on regulating the same two indicators that its predecessors scrutinized: how much revenue a hospital takes in from patient care (after deducting bad debt and free care expenses), and how much a hospital charges commercial insurance companies.
Every January, the board sets a growth percentage for patient care revenue for the hospital system. The board has been gradually pushing that number downward. For fiscal year 2017, which starts Oct. 1, the growth rate is 3 percent.
“Like last year, we recognize the need for a careful balance of the concerns of Vermont citizens and businesses with the financial health of the hospital industry,” Al Gobeille, the chair of the Green Mountain Care Board, wrote in a letter to hospitals outlining this year’s regulatory process.
In addition to the 3 percent cap, the board then allows hospitals to charge a little extra money to insurance companies in order to re-invest in new initiatives, such as accountable care organizations or payment reform under the proposed all-payer model.
When hospitals take in excess money — as nine did in 2015 — the board, like BISHCA, usually forces the hospital to lower how much it charges insurance companies in the subsequent year. But in 2016, the board did not force UVM Medical Center to follow that process.
In an interview, Gobeille said his board’s strategy has been to regulate the money that hospitals take in for the past three years while working to reform how hospitals are paid. He said the regulation is a constant balancing act among solvency, affordability, quality, and access.
“The Green Mountain Care Board has taken a position to try to work with hospitals to try to reduce the rate of health care spending, specifically in commercial insurance,” he said. “There’s a balancing act. It’s about solvency, affordability, access, and quality. It’s balancing competing priorities.”
Gobeille said the board reviews revenues and expenses of the hospitals, but “The hospitals really do the work. The board is not successful in keeping the hospital solvent. The hospital is. These are giant, giant companies with hundreds, and in a cumulative way, thousands of employees. It is not the case where the board keeps them ‘anything.’”
He pointed to the work his board has been supervising the creation of a regulated monopoly for the health care system that will pay hospitals in a structure similar to a monthly stipend. The board will regulate the newly formed Vermont Care Organization, which is responsible for most of Vermont’s hospital and health care system.
“Nobody has ever been successful in regulating fee-for-service hospitals,” Gobeille said. “You push in a balloon here and the balloon pops up over there.” He said he is concerned about the growth of hospitals “or I wouldn’t be doing the job I’m doing.”
“What does affordable mean?” Gobeille said. “With the way we’ve defined it… we basically said, ‘Hey, let’s have net patient revenue grow closer and closer to gross domestic product and gross state product,’ and we’ve been able to do that.”
Gobeille called himself “a pretty conservative guy” and said “wealth is a judgment” when it comes to hospitals.
Assets

The role of UVM Medical Center
The UVM Medical Center holds the majority of assets in Vermont’s hospital system, according to the data from the Green Mountain Care Board.
The Burlington hospital accounts for about half of the $2.3 billion in revenue from patient care that the board regulates. In recent years the hospital has accounted for somewhere between two-thirds and three-quarters of the total surpluses generated in the same hospital system.
In 2001, the UVM Medical Center owned 51.6 percent of assets in the hospital system; that number increased to 55.7 percent by 2016. From 2001 to 2015, UVM Medical Center has been responsible for up to three-quarters of the profits made across Vermont’s 14 hospitals.
The assets were $1.1 billion in fiscal year 2012, $1.2 billion in fiscal years 2013 and 2014, and $1.3 billion in 2015. The profits were $33.6 million in 2012, $42.7 million in 2013, $51.7 million in 2014, and $75.6 million in 2015.
Those numbers also make the hospital wealthier than its counterpart, Dartmouth-Hitchcock Medical Center in Lebanon, New Hampshire. At the end of June 2015, Dartmouth had 135 days cash on hand—62 days less than UVM had that year—and a $3.6 million operating surplus, according to a spokesperson.
Dartmouth’s gross revenue and total assets, however, were higher—at $3.3 billion and $1.5 billion, respectively. UVM received $2.5 billion in gross revenue in fiscal year 2015 and owned $1.3 billion in assets. However, because Dartmouth’s data comes from a different source than UVM’s, it may not be directly comparable.
Additionally, hospitals in the region—Massachusetts General Hospital in Boston, Maine Medical Center in Portland, and Albany Medical Center—did not respond to VTDigger’s inquiries for similar financial data. The information available on their public tax returns may be calculated differently from the Green Mountain Care Board’s data.
Del Trecco, from the hospital association, said looking at historical hospital data can set up an apples-to-oranges conversation. He urged members of the public to focus on the past three or four years of data — when the board has been gradually pushing down hospital revenues.
“I look at all hospitals, not only from historic highs and lows, but sort of the cyclical nature at times of hospital budgets, and the variability from year to year,” Del Trecco said. “I look at the net patient revenue … that’s the money that a hospital would put in their bank account for treating patients.”
Types of revenue
Todd Keating, the chief financial officer for the UVM Health Network, a four hospital group in Vermont and New York, said the operating margin for the Burlington hospital has gone up because of an increase in the number of patients.
“We have been the beneficiary of some significant volume growth over the last five years, and what we’ve been able to do is see a lot of patients without an increase to our fixed costs,” he said. “That also helps contribute to the margin.”
Because it is a 501 (c)(3) nonprofit organization, the UVM Medical Center needs to have a plan to reinvest any annual profits back into the facility. The money often goes to new equipment and modernizing facilities, Keating said.
Over the past decade, some of the hospital’s major projects have included an upgraded birthing center where new dads can stay overnight with the new mom, and a rebranding campaign for the UVM Health Network.
UVM Medical Center has also been filling cash reserves to improve its credit rating with Moody’s. The rating agency requires the hospital to have large amounts of cash in order to handle upcoming payment reform.
The increased cash reserves also allow the hospital borrow at low interest rates because it proves to creditors they can pay their bills. In recent years, Keating said the hospital has been able to refinance debt to save money for the hospital.
Keating said the hospital has also been making investments in community organizations as it prepares for an all-payer model. “We make investments in what we think are the things that we need to do to transition from the fee-for-service world to population management,” he said.
In the upcoming fiscal year 2017, the hospital will ask for a 3 percent increase in how much it charges insurance companies, plus 0.4 percent to re-invest in health care reform. If regulators approve the proposal, the price increase would be the hospital’s lowest price increase since the 1990s, Keating said.
He said the hospital has figured out how to limit price increases to 3 percent because it negotiates low-priced contracts with vendors, such as medical equipment companies, despite the fact that pharmaceutical prices go up 8 to 10 percent every year.
Limiting price increases from companies that supply products is called supply chain management, and in 2015, a national association ranked the hospital No. 2 among academic hospitals in how it manages its supply chain.
Keating said Vermont is a “very low-cost health care provider” compared with the hospitals that he used to manage in Massachusetts, but “we still have to put our nose to the grindstone to continue to squeeze out dollars.”
He pointed to his experience sitting on the board of the Greater Burlington Industrial Corporation, the nonprofit economic development organization for Chittenden County, and said he hears a lot about high insurance premiums.
“I hear the small businesses and the pain that the commercial lifts are,” Keating said. “We’re trying to keep our commercial lifts as low as possible so that pain doesn’t get passed on to the small businesses in Vermont.”
Hearings on hospital budgets for fiscal year 2017 will take place Aug. 17, 18 at the Sheraton Hotel in Burlington and on Aug. 24, and 25 at the Capitol Plaza in Montpelier. They are open to the public.
Cash on hand
