With the second oldest population in the country, Vermont needs its nursing homes. Yet, while Vermonters rapidly age, the state’s long-term care capacity has dwindled, losing 900 beds in the last two decades.
To keep the struggling system afloat, the state has bailed out nursing homes with around $38 million in state and federal Medicaid dollars for so-called extraordinary financial relief over the past five years, according to records obtained by VTDigger.
The practice, which has not previously received media attention, has drawn scrutiny from lawmakers, who this year asked for comprehensive reports and payment records from state leaders regarding the bailout program.

For their part, state health officials say Vermont’s nursing homes are a vital piece of the eldercare landscape. Without extraordinary financial relief, they say, the state would have lost even more critical bedspace.
Efforts to address the upstream causes of the nursing homes’ financial crises, like the state’s reliance on traveling nurses, have received far less financial support.
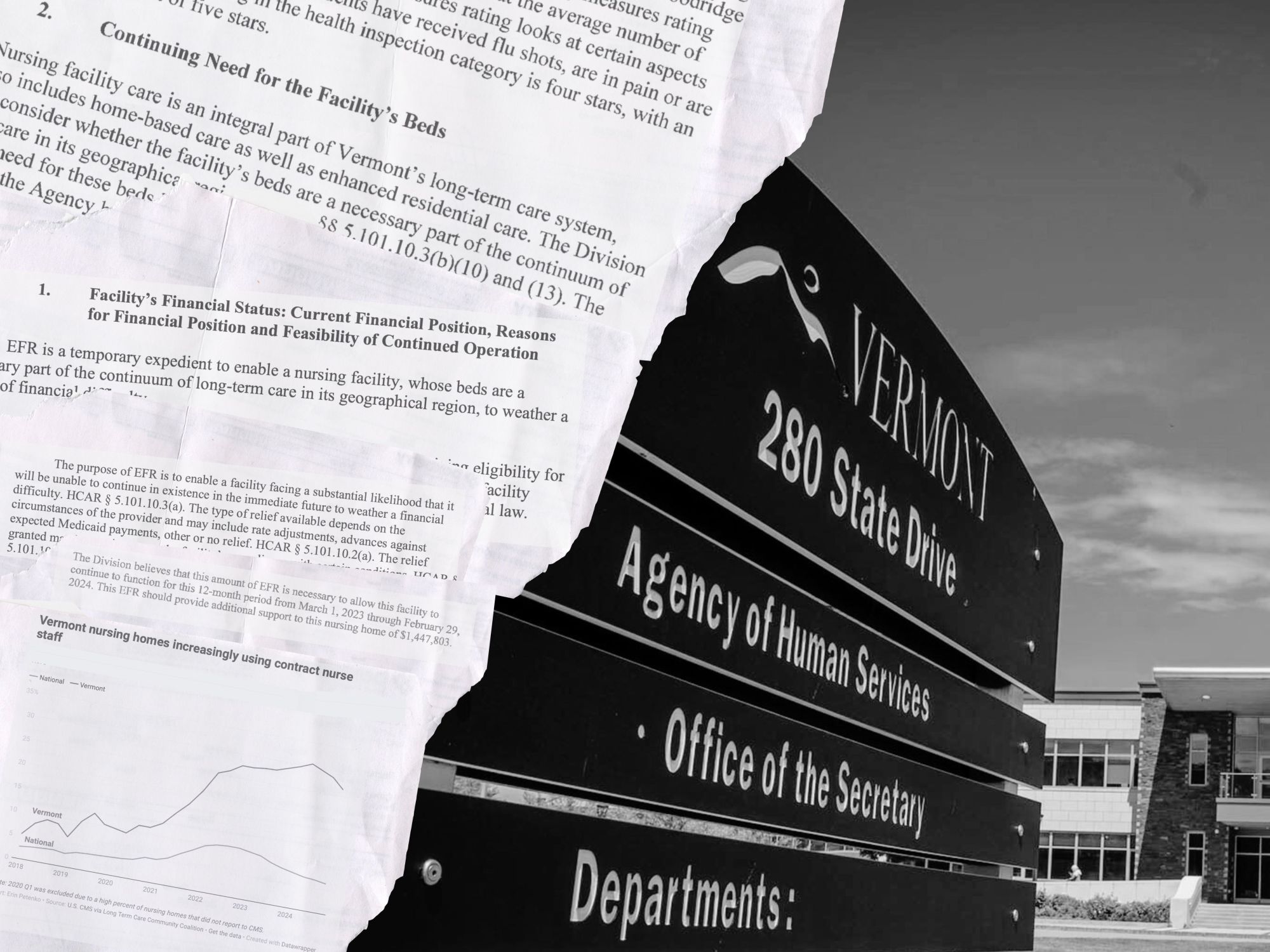
Around half of the extraordinary financial requests from 2020 onward mention concerns with increased costs of staffing, particularly contract staffing. Staff and contract staff make up about 50% of total costs in nursing homes’ budgets, according to the state.
Vermont’s nursing homes depend on traveling staff more than those in any other state, according to federal data from the Centers for Medicare and Medicaid Services.
There are many reasons extraordinary financial relief is not a sustainable means to “plug the gap” for nursing homes, “but we needed something,” said Helen Labun, the Vermont Health Care Association’s executive director.
“We don’t want EFR to be a standard option,” Labun said. “It really is meant to be an extraordinary measure.”
An old program meets an urgent need
Despite existing for more than 20 years, Vermont’s extraordinary financial relief program started playing a recurring and sustaining role for the state’s nursing homes only since the Covid-19 pandemic.
The bureaucratic program routes through multiple departments nested within Vermont’s Agency of Human Services.
The Department of Vermont Health Access’s rate-setting division, which sets Medicaid reimbursement rates for nursing homes, reviews requests submitted by facilities. But the funds for extraordinary financial relief come from Medicaid dollars allocated through the Vermont Department of Disability, Aging, and Independent Living, according to the department’s commissioner, Jill Bowen.
Nursing homes, which receive extraordinary financial relief, provide the most intense level of care, serving people who wouldn’t have their needs met in an assisted living or residential care home, according to Labun. These facilities must serve patients on Medicaid to qualify for financial relief, she said.
There are 33 nursing homes in the state, with a total of about 2,847 beds as of July, a decline of nearly 900 beds in the last 20 years, according to the Department of Disabilities, Aging and Independent Living.
Bowen said the loss of beds in long-term care facilities in the state is worrying given Vermont’s aging demographic, though she said the trend may partially stem from people seeking at-home care instead.

Angela Smith-Dieng, director of DAIL’s Adult Services Division, said the state does not want to lose options for its large elderly population, so extraordinary financial relief is “incredibly important as a tool to prevent nursing home closures.”
One factor leading to increased emergency funding requests, according to state leaders, is the “rebasing” of Medicaid reimbursements. Rebasing, which most recently has occurred in 2025 and 2023, according to state leaders, changes Medicaid reimbursement rates based on cost data from earlier years. In 2023, the state altered reimbursement rates based on 2020 costs, which didn’t yet capture the new financial pressures brought on by the pandemic.
In July, the state again balanced reimbursement rates, this time using 2023 costs, which Bowen hopes will limit the need for extraordinary financial relief.
Working with the Legislature, the Department of Disabilities, Aging and Independent Living advocated for changing how much facilities are paid based on their occupancy, reducing penalties for not meeting high thresholds, according to Bowen.

In some instances, the state has advanced nursing facilities money through the bailout process or provided more money than a facility requested. The state may advance facilities funds if they will not be able to meet payroll for staff, Bowen said, but she added that the state was more likely to provide less — not more — than a company wanted.
The state has recouped every advance back or was in the process of recouping them, according to the department’s rate setting division.
As part of an extraordinary funding review, Jaime Mooney, the director of the rate setting division, said the state examines a company’s finances and whether facilities are in compliance with state and federal requirements.
After the rate setting division reviews the request, combing through the provided financial information like past-due invoices and the amount of cash on hand, the division makes a recommendation to the Department of Disabilities, Aging and Independent Living.
The rate setting division also consults with DAIL regarding possible issues with the care provided by the requesting facility. But Mooney said she couldn’t recall ever denying a facility’s request due to the quality of care.
If a request is granted, the state restricts the grant’s use, and facilities cannot pay penalties or exorbitant owner-administrator fees using the financial relief funds, according to Mooney.
Once granted, the facility must meet reporting requirements, including providing updated financial information, she said.
According to Labun, nursing home owners need to demonstrate they don’t have money from other sources. That prevents companies that own many facilities from shifting their investments to out-of-state homes and then requesting bailouts from Vermont.
In the past, nursing homes had savings they could rely on when reimbursement rates weren’t covering expenses, Labun said. But, during the Covid-19 pandemic, nursing homes’ coffers ran dry, and extraordinary financial relief was retrofitted to respond to the emergency at nursing homes, Labun said.
‘Outlier state’
Nursing homes typically used extraordinary financial relief in one-off cash flow emergencies to “fight financial storms that they might not otherwise have been able to weather,” according to Labun.
That’s now changed, and the cost of nursing is driving the crunch.
Contract staff tend to cost facilities at least twice as much as permanent staff, contributing to nursing homes’ financial distress, Labun said. The use of contract staff in Vermont has fallen slightly, according to Centers for Medicare and Medicaid Services data. But the state’s rate is still exceedingly high compared with the national average, and it has yet to be seen whether this downward trend continues, Labun said.
“Vermont’s an outlier state in terms of our use of travelers as part of a normal part of the workforce,” Labun said.

While the nation saw heightened rates of contract staff at the onset of the Covid-19 pandemic, the rates have generally returned to the pre-pandemic norm, said Richard Mollot, executive director of the Long Term Care Community Coalition, a national nonprofit organization. That’s not the case in Vermont.
Vermont nursing homes had the highest rate of contract staff employment compared to those in other states in 2024, peaking at 31% in the first quarter of 2024, according to analysis of Medicaid data by the Long Term Care Community Coalition. The national average in the same period was 8%.
Mollot, an advocate for nursing home residents, said nursing homes often use a larger number of contract staff when there is high attrition among permanent staff, which is often a result of poor working conditions such as workplace hazards or low pay.
Staffing tends to be the highest expenditure for nursing homes, and oftentimes nursing homes that work with temporary staffing agencies are contractually obligated to pay contract staff more than permanent staff, said Kaili Kuiper, Vermont Legal Aid’s long-term care ombudsman. That means nursing homes spend much of their budget on filling the staffing gap with temporary staff, and do not have the funds to invest in recruiting long-term staff.
This is a “difficult cycle to break, because there’s only so much money to go around,” Kuiper said. The cycle can also cause poor care, and Kuiper said her office has seen “a lot of issues that are related to there not being enough staffing to provide the care that’s needed,” including problems with response times and hygiene.
Not a sustainable means to ‘plug the gap’
Vermont’s demographic challenges are driving the underlying problem of nursing homes’ high use of contract staff, Labun said.
So, in recent years, the Legislature has allocated some funds to rebuild the nursing workforce.
The state put half a million dollars toward attracting and keeping licensed nursing assistants in the current fiscal year budget. That investment was an attempt at addressing the upstream causes of nursing homes’ financial woes, according to Sen. Richard Westman, R-Lamoille, who sits on the Senate Appropriations Committee and serves on the board of a rural hospital.
The state plans to draw down federal funds for workforce development from the Civil Monetary Penalty Reinvestment Program that had previously been held up in between the President Joe Biden’s and President Donald Trump’s administrations and during the federal shutdown, Labun said.

The legislative investment was far less than the money spent on extraordinary relief, but Westman argued that prioritization makes sense, given the financial weakness of some facilities. In the last two years, about two-thirds of nursing homes have requested extraordinary relief, he said in a May interview.
“I think one could make an argument that without that help, they probably would have gone out of business,” Westman said.
Staffing underlies the financial challenges, Westman said, echoing others. Investing in nurse recruitment and retention, as well as increasing reimbursement rates nursing homes receive, could prevent the facilities’ reliance on bail out money, he suggested.
Kuiper said that using temporary emergency staff is an important tool. As the state’s advocate for nursing home residents, Kuiper said employing contract staff is a better alternative than allowing a facility to be understaffed.
But in the long run, Kuiper said she would like to see “a stronger movement away from temporary staff,” and for the care community to prioritize strategies to curb the high use of contract staff as the “status quo.”
Former VTDigger reporter Peter D’Auria contributed reporting.