
[N]orthwestern and central Vermont are the healthiest areas of the state, while the Northeast Kingdom and southern Vermont continue to lag, according to statistics in a new national study.
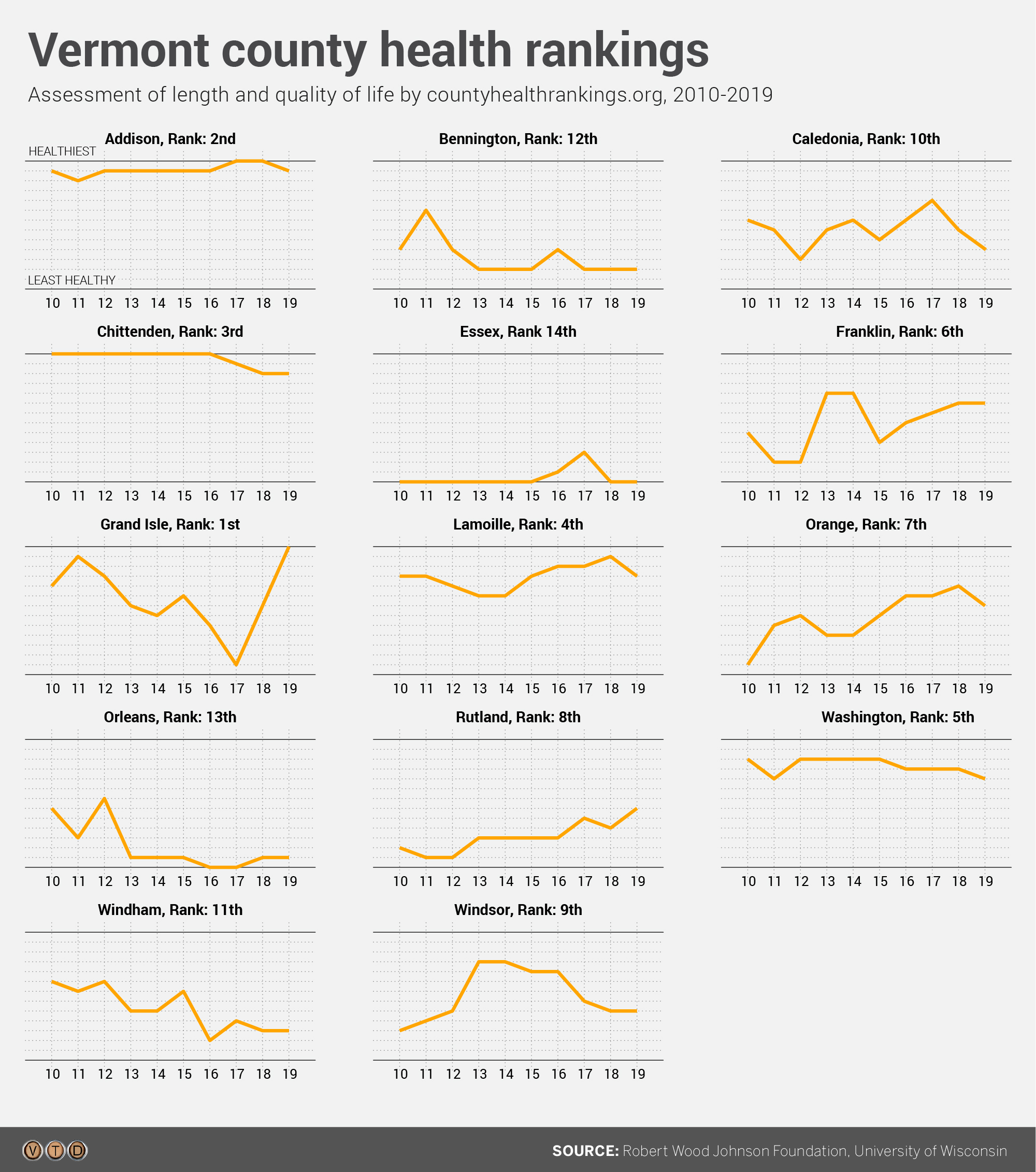
The county-by-county report, from the Robert Wood Johnson Foundation and the University of Wisconsin Population Health Institute, pegs Grand Isle as the healthiest county in Vermont. For the second year in a row, Essex is the least healthy.
The geographic trends are not new and not surprising, given the deep-rooted demographic issues that influence health rankings, Green Mountain Care Board Chair Kevin Mullin said.
“That doesn’t mean we shouldn’t be trying to (change) it, though,” Mullin said. “Because otherwise, the next generation will be grappling with the same issues.”
The new Vermont report examines a long list of issues under two broad categories – health outcomes and health factors.
The study’s primary measurement is health outcomes, which represents “how long people live and how healthy people feel,” the authors of the report say. By that measure, the top five counties were Grand Isle, Addison, Chittenden, Lamoille and Washington.
Addison was the healthiest county in last year’s report. All of this year’s top five, aside from Grand Isle, also made the top five on last year’s list.
On the other end of the spectrum, the bottom five counties for 2019 were Caledonia, Windham, Bennington, Orleans and Essex. The bottom four were the same in the 2018 report.
One key measurement of premature death – which calculates years of life lost before age 75 – shows the big disparity between the top and bottom of the list. The rate was 3.5 times higher in Essex County than in Addison.
Also, Essex County had the highest portion of adults – 16 percent – who reported they were in poor or fair health. At the low end, 10 percent of adults fell into that category in Chittenden and Washington counties.
Also, Essex and Orleans counties had the highest rate of “poor mental health days.” Chittenden and Grand Isle were the lowest in that category.
The report’s findings were somewhat different when the counties were ranked by health factors. Those factors include health behaviors like alcohol and tobacco use; clinical care issues including access and quality; socio-economic factors; and the physical environment.
However, same general geographic trends prevailed. The top five counties in terms of health factors were Chittenden, Addison, Washington, Windsor and Grand Isle; the bottom five were Rutland, Bennington, Caledonia, Essex and Orleans.
Other measures showed how far apart the counties were. The teen birth rate in Orleans was 27 per 1,000 females between ages 15-19; the rate was just six per 1,000 in Chittenden and nine per 1,000 in Addison.
Various Northeast Kingdom counties also ranked highest in the state for adult smoking, children in poverty, food insecurity and diabetes while scoring low in median household income and the number of primary care providers in relation to population.
The authors of the study also focused on housing costs this year: They said 56 percent of Vermont’s children in poverty live in a household where more than half of the income goes toward housing costs.
The report also found racial disparities. While 16 percent of Vermont households spend more than half of their income on housing, that percentage was significantly higher for black households and American Indian/Alaskan native/Native American households.
“Our homes are inextricably tied to our health,” Robert Wood Johnson Foundation President and Chief Executive Officer Richard Besser said in announcing this year’s report. “It’s unacceptable that so many individuals and families face barriers to health because of what they have to spend on housing. This leaves them with fewer dollars to keep their families healthy.”
Mullin made a similar connection between health and demographic factors in the report.
“The more rural the area, with less economic opportunity, then you have more alcohol use, you have more obesity, you have more smoking, which in turn leads to worse health outcomes,” Mullin said.
“I don’t think it’s any surprise – it’s something we’ve heard from hospitals repeatedly,” he added. “It’s hard to argue with them. The question is, how do we change those demographics.”
Mullin cited the state’s ongoing all-payer experiment in health reform as one way to tackle the issue. “Can we do things differently and try to do more with prevention and wellness, and not just treat people when they’re sick?” he said.
The RiseVT program is attempting to combat the state’s obesity issues.
Vermont Health Commissioner Mark Levine pointed to the State Health Improvement Plan, which “focuses on making sure that everyone in Vermont has a fair and just opportunity to live a long and healthy life.”
“To accomplish this, we are very deliberately working with our community and other partners to address the root causes of health inequities,” Levine said. “This will require us to continue zeroing in on opportunities for improving health outcomes through housing, transportation and food and economic security initiatives.”