
Editor’s note: VTDigger’s investigation, Medicaid by the Numbers, draws on data from the Department of Vermont Health Access, the Legislature’s Joint Fiscal Office, the U.S. Census Bureau and other relevant sources. In some cases, VTDigger found it difficult to obtain data, and has sought to make that clear to readers wherever appropriate. The series started March 6 and will continue over the next several weeks. Find all of the stories here.
[O]ver the past decade, enrollment has nearly doubled in health care programs Vermont pays for with Medicaid money.
As of 2015, about one-third of Vermont’s population used some kind of program funded through Medicaid dollars.
A VTDigger analysis shows that the increase is likely related to a combination of factors, including demographics, income changes and new eligibility rules.
Compared with the rest of the nation, Vermont has a relatively high population of people who are aged and disabled. The state expanded health care access at the beginning of the Great Recession, when incomes were dropping. And the expansion of Medicaid under the Affordable Care Act changed the way the state determines program eligibility.
Steven Costantino is the commissioner of the Department of Vermont Health Access, the agency of state government that acts as the health care insurer for low-income people. The department is responsible for overseeing about half of Medicaid spending in Vermont.
Costantino told the House Appropriations Committee in December his theory for why Medicaid enrollment has increased. “The biggest driver in Medicaid budgets as you know is a thing that we call caseload,” he said. “That’s the number of people on Medicaid and how often they use the service.”
He said there could be two changes driving increase: slow economic growth that forces people onto not just traditional Medicaid, but also human services supported by Medicaid; and a change in the way the Affordable Care Act determined income elibility for the program.
Under new rules, which allow more exemptions for income, more people qualify for the program. Costantino cited “a shift” of individuals making between $16,000 and $35,000 who moved from private insurance over “to the regular Medicaid program.”
“The other thing you look at is the overall economy of the state,” Costantino said. “If your overall economy is not growing, people just tend to be eligible for Medicaid.”
VTDigger obtained enrollment data from the Department of Vermont Health Access and compared the state data to public data from the U.S. Census Bureau, which collects demographic information.


The data analysis yielded three main findings.
1: There is a general upward trend in aged, blind, and disabled adults using Medicaid. This may correlate with the fact that Vermont is an aging state. Further, data from the U.S. Census Bureau shows that Vermont has a slightly higher-than-average percentage of people under 65 living with disabilities.
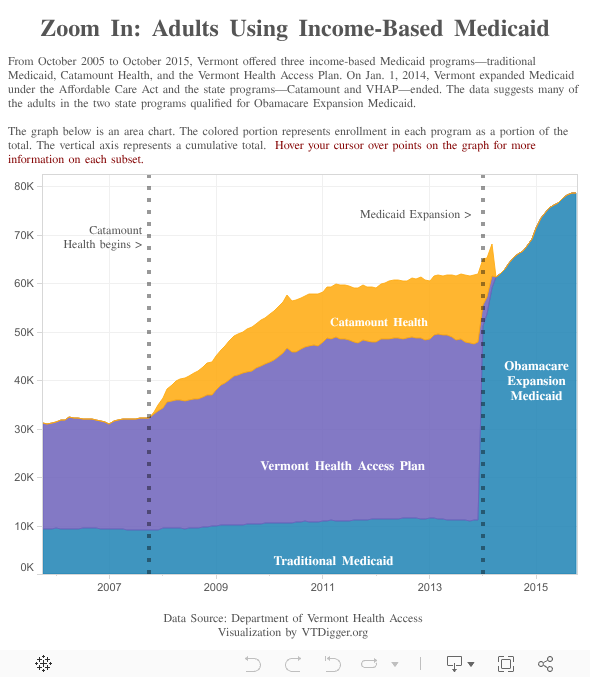
2. In late 2007, at the same time the nation was slipping into a recession that spurred major job losses, Vermont expanded income-based health care coverage through a program called Catamount Health. Adult enrollment skyrocketed. By 2011, adults using income-based Medicaid programs exceeded children on income-based Medicaid programs, even though eligibility rules make it easier for children to enroll in the program.
3. In early 2014, Vermont expanded Medicaid under the Affordable Care Act. Vermont already had some of the most generous Medicaid programs in the nation, and had a significant number of adults using income-based Medicaid programs. But the Affordable Care Act changed the eligibility level to qualify for Medicaid from 100 percent to 138 percent of the poverty level—or about $12,o00 to $16,000 for a single person.

Before 2014, the lowest-income residents used the Vermont Health Access Plan, a state-run program that was very similar to traditional Medicaid. Applicants to VHAP were required to declare all income sources.
Lower-middle-income Vermonters often ended up on Catamount, which covered people making up to 300 percent of the poverty level, or, for a single person, about $35,000 in 2015. Catamount, signed into law by Gov. Jim Douglas, was essentially a private-public partnership. Qualifying residents could buy private insurance through the state’s Medicaid office, and Vermont subsidized their insurance.
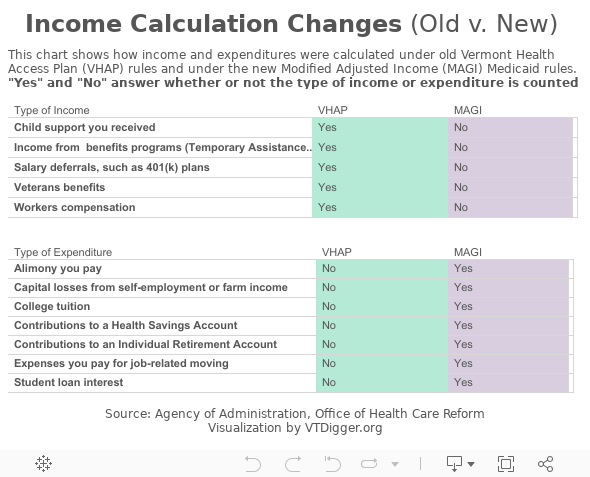
When the Affordable Care Act allowed states to expand Medicaid, the federal government also changed income calculations for eligbility. Vermonters seeking to use traditional Medicaid now could declare fewer sources of income and deduct more expenses.
Under the new formula, income from child support and worker’s compensation are not considered income. Additionally, applicants can deduct expenses such as college tuition, contributions to certain retirement accounts and alimony paid to former spouses.
Health care experts in Vermont say the income rule changes likely resulted in a dramatic increase in enrollments in income-based Medicaid programs. Data analyzed by VTDigger shows that the enrollment of adults in income-based Medicaid programs increased from about 63,000 at the beginning of 2014 to nearly 79,000 in October 2015—the sharpest increase for that population group in the decade studied.
People who qualified for the Vermont Health Access Plan were forced to move over to the expanded Medicaid program if they wanted state health insurance. The state also expected people using Catamount Health to transfer to Vermont Health Connect’s subsidized private insurance, but both experts and data show that many Catamount customers transferred to the new Medicaid program.
About 19,000 people receive subsidies from Medicaid for the Vermont Health Connect program, which is comparable to the now-defunct Catamount Health plan, which had about 14,000 enrollees. People who receive the subsidies are considered direct enrollees, even though they are not using a traditional Medicaid program.

There is no specific type of person who uses a Medicaid program, says Trinka Kerr, the chief health care advocate at Vermont Legal Aid. She described people who qualify for Medicaid as “all over the map” and said they include farmers and small business owners.
“As a result of the ACA, they changed the methodology for determining eligibility,” she said. “It used to be there were very specific things that were included when you talked about income, and under the Affordable Care Act, they look at modified adjusted gross income, which is based on your taxable income, which is a completely different system.”
Self-employment income is particularly difficult to gauge, Kerr said. State officials may have misjudged the types of income and expenses of self-employed Vermonters, or “may have miscalculated how many people in Vermont are self-employed, and therefore benefited from (modified adjusted gross income),” she said.
“Maybe they didn’t understand the nature of the state’s economy,” Kerr said. “There’s farmers. There’s people starting their own little boutique businesses. And I think that group is kind of large in Vermont.”
The good news about Medicaid expansion, Kerr said, is that her office gets fewer calls from people concerned about the cost of health care.